Case Report
Neonatal Abstinence Syndrome in a Newborn With Osteogenesis Imperfecta With Fractures
By Genevieve D’Souza, MD and Rita Agarwal, MD, FAAP
Lucille Packard Children’s Hospital, Stanford
Neonatal abstinence syndrome (NAS) occurs in newborns after in-utero exposure to opioids. In the United States, the incidence of NAS increased 383% from 2000–2012. Management of these patients may be complicated by use of illicit drugs as well as potentially ongoing pain problems. The cost of treating these babies in the short term is soaring (Cost and incidence of NAS 6/2017); long term costs and medical problems are still evolving. We discuss a case of a baby with NAS and review management principles.
Case
Ex 34-week infant who was born to a mother with a history of severe Osteogenesis Imperfecta (OI) and chronic pain.
Mother on methadone 15mg TID during the pregnancy for her chronic pain and PRN. Her hydrocodone/acetaminophen dose had been weaned from a higher dose of 100 mg/day earlier in pregnancy to 30mg/day in an attempt to limit fetal exposure.
Fetal ultrasounds showed limb length less than expected for gestational age and evidence of in-utero rib and limb fractures. X-rays at birth revealed healing femur fractures. The inpatient pain service was consulted for evaluation and treatment of NAS and ongoing pain issues. The baby was started on morphine 50 mCg/kg IV every two hours or 100mCg/kg PO every two hours as needed for pain or withdrawal. Acetaminophen was added for breakthrough pain and pain and withdrawal scores were carefully followed and documented. The baby was worked up for fractures and diagnosis of OI by the primary team.
Discussion
Neonatal abstinence syndrome occurs in babies either after delivery from a mother who was using opioids during her pregnancy, or after discontinuation of opioids used during the course of medical treatment. Opioid use during pregnancy is associated with intrauterine growth retardation, prematurity and small for gestational age infants. The signs and symptoms are the same in both cases and include:
- High-pitched cry
- Jitteriness
- Tremors
- Generalized convulsions
- Sweating
- Fever
- Mottling
- Excessive sucking or rooting
- Poor feeding
- Vomiting
- Diarrhea
Diagnosis can be complicated by the fact that mothers often underreport or deny their use of opioids. NAS should be suspected in babies who present with the above symptoms or excessive rooting/sucking, sneezing or yawning.
Methadone is a long acting opioid that crosses the placenta, and has been used since the 1960s. Its plasma levels in cord blood are five times lower than maternal blood and neonatal effects may be less dramatic than other opioids. The half-life of methadone in the neonate is prolonged to approximately 32 hours. A baby born after methadone exposure may show signs as early as 48 hours after birth, but may not show signs of NAS until 7-14 days after birth. There is evidence that some may not show signs until four weeks after birth and subacute signs can occur for as long as six months. Premature and younger gestational age infants have fewer signs of NAS.
In addition, a baby with evidence of ongoing pain sources (healing or new fractures) will need ongoing pain management that may not be covered by methadone blood levels.
Methadone may be transferred in maternal breast milk at a variable rate, and the literature suggests on average of only 3% of the maternal dose is available.
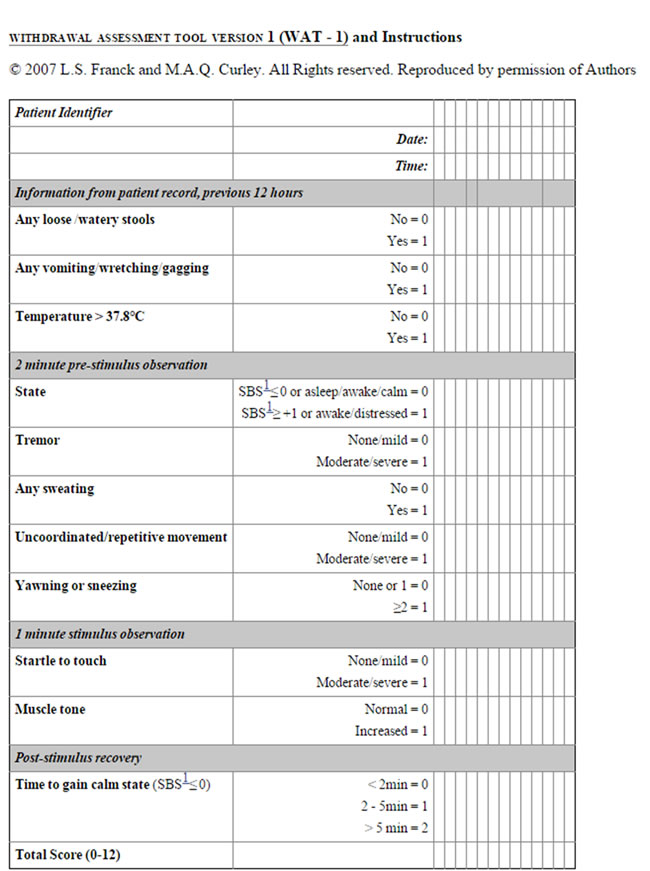
Designing a plan to treat pain and withdrawal requires careful consideration of the sources of opioids and close monitoring of both withdrawal scores and pain scales. One of the commonly used scales is called the WAT score (below).
WAT score - A total score greater than three indicates withdrawal
For babies who will not be breast fed or whose mothers will discontinue opioid use, babies can be weaned slowly. However, for a mother who is on ongoing opioid treatment such as methadone, and plans to breast feed, it is important to discuss the mother’s opioid use and advise her regarding sudden increases or decreases in use, and her breastfeeding plan.
When she is ready to wean breast milk, she should wean the volume off slowly to prevent withdrawal in infant.
Parents should be cautioned to watch for sudden changes in infants; consumption of breastmilk (and thus small but steady methadone) intake, excessive sleepiness, small pupils, dilated pupils, excessive fussiness or other withdrawal symptoms.
References
- Neonatal Abstinence Syndrome. Kocherlakota P. Pediatrics Aug 2014, 134 (2)
Breastfeeding and Methadone Therapy: The Maternal Experience. Demirci JR, Bogen DL, Klionsky Y. Substance Abuse. 2015;36(2):203-8. - Obstetrical and neonatal outcomes of methadone-maintained pregnant women: a Canadian multisite cohort study. Ordean A, Kahan M, Graves L, Abrahams R, Kim T. J Obstet Gynaecol Can. 2015 Mar;37(3):252-7.
Question: Is breastfeeding useful in the management of neonatal abstinence syndrome? Lefevere J, Allegaert K Arch Dis Child 2015;100:4 414-415
![]()