3D Printing and Pediatric Pain Management: Hype or hope?
 By James Mooney, MD
By James Mooney, MD
Penn State Milton S. Hershey Medical Center
In recent years it’s been difficult, if not impossible, to avoid being exposed to the topic of 3D printing. From prosthetics for children with missing limbs, to wrenches produced on board the International Space Station, the popular news is rife with representations of these technologies. But popular news is just that: popular. It can have little relevance to the practice of pediatric pain medicine. The purpose of this article is to provide insight into some of the technologies being discussed and highlight how they may affect your acute and chronic care patients and practice in the not so distant future. While a ‘how-to’ on building a human head (Figure 1) might be interesting, it wouldn’t illustrate the breadth of the technologies very well. Rather, these issues will be presented using the perspectives of the underlying sciences, the educational and pre-clinical arenas and finally the current and future direct clinical use. First a clarification of the technologies and terminology is necessary.
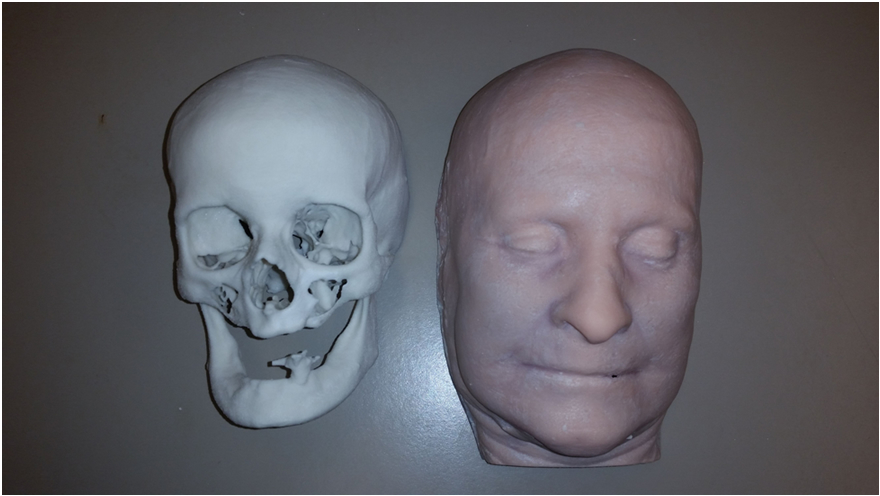
Figure 1
Technologies and Terminology
3D printing, additive manufacturing, rapid prototyping and several other terms are often used in vague and almost interchangeable ways. Contrasting a few mental models can be useful to sort many of these things out.
Traditional manufacturing, involving producing thousands to millions of identical widgets, can be contrasted to what may be called “rapid prototyping”, “rapid manufacturing” or “bespoke production” among other names. These techniques produce low volumes (sometimes one object, other times 100) and may or may not produce any identical copies of a particular widget. For the rest of this article I will use the term rapid prototyping (RP) for these processes.
Both traditional manufacturing and rapid prototyping may use what are called additive or subtractive manufacturing technologies. Subtractive manufacturing begins with a bulk of material, from which bits are removed to produce the final product. A fine example of this would be producing a wooden bowl from a solid tree trunk on a lathe. Additive manufacturing, by contrast, begins with a blank slate (often quite literally) and adds material to produce the final product. 3D printing is the most familiar example of this, though even that term encompasses many technologies. Due to intellectual property concerns, branding, etc. there are numerous terms, but a standard terminology for additive manufacturing (designation F2792-12a) has recently been developed by ASTM International (formerly known as American Society for Testing and Materials). The various standard terms are illustrated in Figure 2 (courtesy Chris Thompson of NextFab, Philadelphia). For reference, most consumer/office grade printers use either material extrusion or vat polymerization.
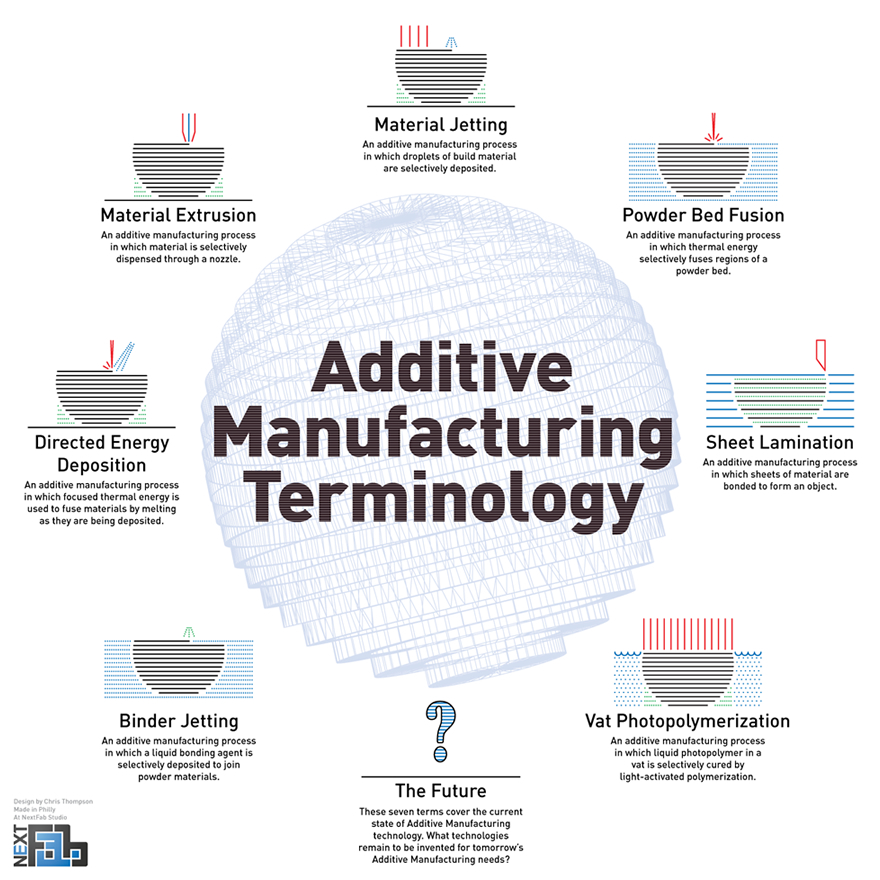
Figure 2
So, what technologies are involved in rapid prototyping besides 3D printing? The main techniques are CNC (Computer Numerical Control) milling, vacuum forming, molding/casting and laser/water jet cutting. CNC milling is computer controlled removal of material, using high speed bits similar to those in a drill or router. As the name implies, vacuum forming uses vacuum pressure to form heated plastics around molds. Molding & casting is the process of making a form (mold) and filling it (casting) with material desired to be in that shape. Laser or water jet cutting uses computer controlled machines to cut (generally) flat materials, though with creative cuts or advanced machines a third dimension to the materials may be added. Frequently these techniques are combined to create the prototype or product with the desired characteristics.
So far I haven’t mentioned the one technology that may be most prominent in the common perception of 3D printing: Bioprinting. This involves the production of living tissues, often utilizing several techniques in combination. For example, a matrix may be 3D printed which is seeded with cells then bathed in a nutritive, growth promoting medium. The ‘holy grail’ of bioprinting, however, is the deposition of organ specific cells, connective tissues and supporting vascular structures in a single process to rapidly create a functioning organ, whether it be skin, liver, or other organs.
Determining what shapes are needed and how to develop these shapes would vary by the desired outcome, of course. But in healthcare we frequently have imaging data that defines the exact physical structure of our patients. With the right software DICOM (Digital Imaging and Communications in Medicine) files from MRI, CT or even ultrasounds can be modified and converted (Figure 3) into standard file formats that can be sent to 3D printers or CNC milling machines. Generally, the amount of detail a milling machine or 3D printer is capable of producing is far greater than the imaging files contain. Even home-made 3D printers are capable of accuracy below tenths of millimeters, but MRI slices are a millimeter thick or more.
Figure 3
Underlying Science
The research arena holds some of the most exciting as well as some of the most seemingly mundane applications of rapid prototyping.
Early bench or clinical research may be significantly improved with the use of equipment produced using RP. Some of this might be customized equipment (such as in microfluidics), it may simply be cheaper than purchasing commercial products, or it may be new methods of testing and validating results. These techniques may allow more research to be performed, with more duplication of results using consistent equipment leading to better scientific foundations of our care. As an example, at my own institution, we are currently working on a project evaluating epidural catheters that relies on an acrylic frame created using a laser cutter (Figure 4, inset showing detail of pieces). When we publish the results of this work, we can also release the files used to create this frame.
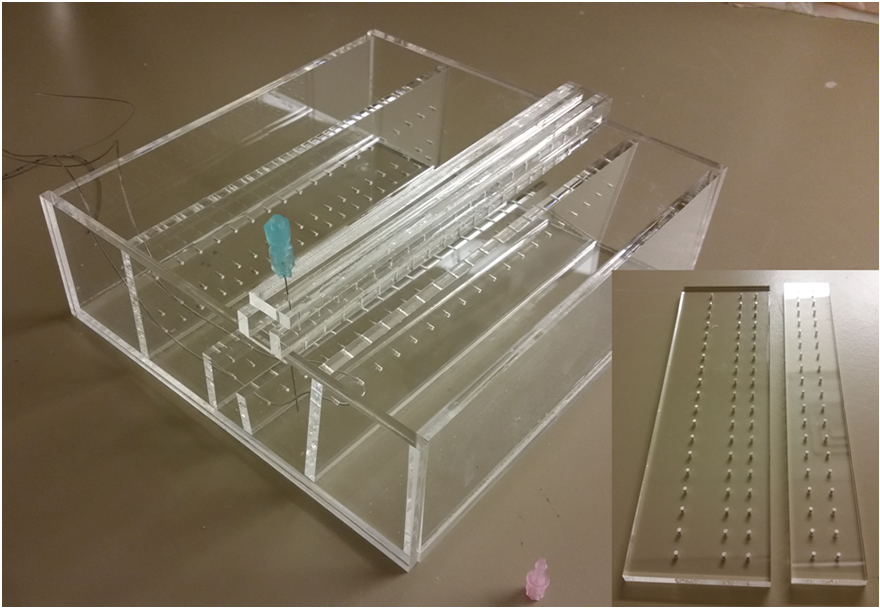
Figure 4
This area has also seen a fair amount of open source distribution of the developed tools. The open source 3D printing movement has been hailed for democratizing production, and may democratize research. One example of this is the NIH 3D Print Exchange website (http://3dprint.nih.gov/).
Perhaps not surprisingly, rapid prototyping and 3D printing techniques are being researched in drug and device development. Surgical (and other) device development has attracted a lot of attention as well. Rapid prototyping technologies can allow for creation of structures too complicated to produce in a viable product or that are simply not possible otherwise. This may lead to interventional pain procedures that, rather than relying on a narrow trajectory free of vital structures, allow us to navigate a flexible device around structures, akin to laparoscopic devices.
Recent releases of viable liver tissue for research has opened the possibility of applying large varieties of compounds to complex tissue systems to screen for results, desirable or otherwise. Extension of the idea of bioprinting complex systems could allow us to essentially perform in vivo research in an in vitro fashion by ‘printing’ significant portions of complicated nervous systems. This however begins to raise significant ethical and moral questions of research and life.
Educational and Pre-clinical
The educational role of open source 3D printers is often discussed in the press. Application of the products of these printers, and other RP technologies, to medical sciences holds quite a bit of potential. Anatomic specimens that may be unique and unavailable to the majority of healthcare students may be reproduced for broader consumption with these techniques. A ‘hands-on’ experience may be feasible with many more models than are currently available and unique ways of presenting the anatomy may be developed for specialized applications. Being able to hold an accurate presentation of the nervous system (for example) with customized labeling or coloring and selective inclusion of associated anatomy may do more for understanding than all the imaging slices ever produced.
If this anatomy can be produced, particularly with appropriate mobility and texture, then simulating pain management procedures can be further enhanced. Our own group is working on using casting and molding to modify existing human simulations, as well as combining several techniques to develop an affordable yet accurate caudal epidural model. The next step in these simulant technologies could be patient specific simulations when confronted with difficult anatomy. For example, my colleagues and I are looking at using 3D printed spinal anatomy (similar to the skull in Figure 1) to evaluate potential approaches for interventional techniques in patients with spinal fusions or other difficult anatomy. Based on the existing MRI data, we will be 3D printing the spines of these patients to allow providers to hold the bony anatomy and evaluate needle access options. We hope to show that these models allow us to reduce radiation dosage and discomfort as well as to find approaches for injections where computer imaging alone fails. There is also the option of creating simulations of uncommon pain relieving procedures that may not be a viable market for the larger simulant manufacturers.
It is also becoming clear that there is the potential for these techniques to be used to plan or optimize treatments to reduce side effects/complications and improve outcomes. Space filling models or other techniques may be used to plan reconstructive surgeries, leading to better functional or cosmetic outcomes. Similar models may also be used to optimize radiation therapy by testing the planned regimen. With tumors being reduced in size, but still deadly, clear models which highlight the tumors may be used to guide their surgical removal. Perhaps, these patients with improved treatment may experience less pain to begin with.
Clinical Use
The area where these technologies interact directly with the patient may hold the most interest for the majority of readers. While some things remain relatively far off, other applications are seeing use today.
Perhaps most prominent of the current uses, is in the prosthetics and orthotics arena. Of course, with combinations of techniques comes the potential for much more diverse devices than one would generally think of with 3D printing. Well-functioning home or volunteer made prosthetics are already competing with the utility of commercially made models, and competitive innovation is sure to follow. Early examples include novel splints or casts for orthopedic injuries and in scoliosis. Improved scoliosis bracing, may lead to more patients avoiding the pain and trauma of spinal fusions.
Surgical interventions using innovative approaches and RP may reduce the burden of pain for patients. With the possibility of custom, patient specific vertebral bodies or discs, as well as entire joint replacements designed for an individual, the burden of pain from spine and rheumatologic disease may be entering new phases of treatment. Even such difficult to manage situations as osteonecrosis may see benefit. In addition to the possibility of replacing an entire bone, implants may be designed to fill a necrotic void in the bone. This implant may be a structural replacement meant to be permanent, or a matrix for new bone growth. These implants could even be used in a palliative process, as ‘space filling’ models for comfort in terminal patients.
Bioprinting of course opens up a multitude of possibilities. Most immediately relevant to the relief of pain and suffering might be the possibility of rapidly printing new skin for significant burns, without creating new injuries by harvesting tissue. Extending the idea of suffering to experiencing an inability to breathe, printing new tracheas or lung tissue is one approach being worked on across the globe. While printing significant portions of a nervous system may never be a reality for patients in pain, it might be reasonable to print new limbs for patients with losses due to injury or illness. This then may raise the ethical question of electively amputating a limb to be replaced with a new, non-painful one or even just a ‘better’ performing one.
Patients presenting with existing pain disorders may not be candidates for surgical interventions, even with all these possibilities in RP. There are, however, other new opportunities being made available for them. Rehabilitation approaches may be improved with options as seemingly simple as better sleep due to custom CPAP masks or improved physical functioning with orthotics/prosthetics. While research may lead to new pain models and medications to intervene, even the very tablets we use may be remodeled. Work is underway to develop 3D printed forms of medications to allow unique controlled release methods, as well as ‘on demand’ combinations of multiple medications. Taken to the next level this could allow an entire pharmaceutical regimen to be managed with a single tablet taken daily.
Summary
Any early or innovative use of technology will have a fair amount of hype (https://www.gartner.com/newsroom/id/2819918) and medical applications of rapid prototyping and 3D printing are no exception. What may separate these technologies from ‘flash in the pan’ advances are the breadth of the potential applications and the strength of the academic aspects. Already there is a Master of Bioprinting degree available, and other similar degrees appear to be in the works. It has become a routine tool in engineering programs down to the level of high school classes. New materials and techniques are being actively investigated across the globe, not only for healthcare but also for other industries. This cross pollination will ensure you will be seeing or experiencing significant advances of these technologies in the years ahead. The only real question is: Will we take full advantage of them for our patients?
Bibliography - Journals
(A selection of recent articles on this topic, as examples of the work discussed)
- Castilho M, Moseke C, Ewald A, et al. Direct 3D powder printing of biphasic calcium phosphate scaffolds for substitution of complex bone defects. Biofabrication. 2014;6(1):015006. doi:10.1088/1758-5082/6/1/015006.
- Chae MP, Lin F, Spychal RT, Hunter-Smith DJ, Rozen WM. 3D-Printed haptic “Reverse” models for preoperative planning in soft tissue reconstruction: A case report. Microsurgery. 2014. doi:10.1002/micr.22293.
- Chang JW, Park SA, Park J-K, et al. Tissue-engineered tracheal reconstruction using three-dimensionally printed artificial tracheal graft: preliminary report. Artif Organs. 2014;38(6):E95-E105. doi:10.1111/aor.12310.
- Del Junco M, Okhunov Z, Yoon R, et al. Development and Initial Porcine and Cadaver Experience with Three-Dimensional Printing of Endoscopic and Laparoscopic Equipment. J Endourol. 2014. doi:10.1089/end.2014.0280.
- Dhir V, Itoi T, Fockens P, et al. Novel ex vivo model for hands-on teaching of and training in EUS-guided biliary drainage: creation of “Mumbai EUS” stereolithography/3D printing bile duct prototype (with videos). Gastrointest Endosc. 2014. doi:10.1016/j.gie.2014.09.011.
- Dong J, Zhang S, Liu H, Li X, Liu Y, Du Y. Novel alternative therapy for spinal tuberculosis during surgery: reconstructing with anti-tuberculosis bioactivity implants. Expert Opin Drug Deliv. 2013. doi:10.1517/17425247.2014.872625.
- Frame M, Leach W. DIY 3D printing of custom orthopaedic implants: a proof of concept study. Surg Technol Int. 2014;24:314-7.
- Gear JI, Long C, Rushforth D, Chittenden SJ, Cummings C, Flux GD. Development of patient-specific molecular imaging phantoms using a 3D printer. Med Phys. 2014;41(8):082502. doi:10.1118/1.4887854.
- Goyanes A, Buanz ABM, Basit AW, Gaisford S. Fused-filament 3D printing (3DP) for fabrication of tablets. Int J Pharm. 2014;476(1-2):88-92. doi:10.1016/j.ijpharm.2014.09.044.
- Goyanes A, Buanz ABM, Hatton GB, Gaisford S, Basit AW. 3D printing of modified-release aminosalicylate (4-ASA and 5-ASA) tablets. Eur J Pharm Biopharm. 2014. doi:10.1016/j.ejpb.2014.12.003.
- He Y, Xue G-H, Fu J-Z. Fabrication of low cost soft tissue prostheses with the desktop 3D printer. Sci Rep. 2014;4:6973. doi:10.1038/srep06973.
- Herrmann K-H, Gärtner C, Güllmar D, Krämer M, Reichenbach JR. 3D printing of MRI compatible components: why every MRI research group should have a low-budget 3D printer. Med Eng Phys. 2014;36(10):1373-80. doi:10.1016/j.medengphy.2014.06.008.
- Igami T, Nakamura Y, Hirose T, et al. Application of a three-dimensional print of a liver in hepatectomy for small tumors invisible by intraoperative ultrasonography: preliminary experience. World J Surg. 2014;38(12):3163-6. doi:10.1007/s00268-014-2740-7.
- Lee V, Singh G, Trasatti JP, et al. Design and Fabrication of Human Skin by Three-Dimensional Bioprinting. Tissue Eng Part C Methods. 2013. doi:10.1089/ten.TEC.2013.0335.
- McMenamin PG, Quayle MR, McHenry CR, Adams JW. The production of anatomical teaching resources using three-dimensional (3D) printing technology. Anat Sci Educ. 7(6):479-86. doi:10.1002/ase.1475.
- Moulton SE, Wallace GG. 3-dimensional (3D) fabricated polymer based drug delivery systems. J Control Release. 2014;193:27-34. doi:10.1016/j.jconrel.2014.07.005.
- Murphy SV, Atala A. 3D bioprinting of tissues and organs. Nat Biotechnol. 2014;32(8):773-85. doi:10.1038/nbt.2958.
- O’Neill PF, Ben Azouz A, Vázquez M, et al. Advances in three-dimensional rapid prototyping of microfluidic devices for biological applications. Biomicrofluidics. 2014;8(5):052112. doi:10.1063/1.4898632.
- Patel SR, Ghose K, Eskandar EN. An open source 3-d printed modular micro-drive system for acute neurophysiology. PLoS ONE. 2014;9(4):e94262. doi:10.1371/journal.pone.0094262.
- Priester A, Natarajan S, Le JD, et al. A system for evaluating magnetic resonance imaging of prostate cancer using patient-specific 3D printed molds. Am J Clin Exp Urol. 2014;2(2):127-35.
- Pruksakorn D, Chantarapanich N, Arpornchayanon O, Leerapun T, Sitthiseripratip K, Vatanapatimakul N. Rapid-prototype endoprosthesis for palliative reconstruction of an upper extremity after resection of bone metastasis. Int J Comput Assist Radiol Surg. 2014. doi:10.1007/s11548-014-1072-2.
- Rankin TM, Giovinco NA, Cucher DJ, Watts G, Hurwitz B, Armstrong DG. Three-dimensional printing surgical instruments: are we there yet? J Surg Res. 2014;189(2):193-7. doi:10.1016/j.jss.2014.02.020.
- Skowyra J, Pietrzak K, Alhnan MA. Fabrication of extended-release patient-tailored prednisolone tablets via fused deposition modelling (FDM) 3D printing. Eur J Pharm Sci. 2014;68C:11-17. doi:10.1016/j.ejps.2014.11.009.
- Vaccarezza M, Papa V. 3D printing: a valuable resource in human anatomy education. Anat Sci Int. 2014. doi:10.1007/s12565-014-0257-7.
- West SJ, Mari J-M, Khan A, et al. Development of an ultrasound phantom for spinal injections with 3-dimensional printing. Reg Anesth Pain Med. 39(5):429-33. doi:10.1097/AAP.0000000000000136.
- Xie P, Hu Z, Zhang X, et al. Application of 3-dimensional printing technology to construct an eye model for fundus viewing study. PLoS ONE. 2014;9(11):e109373. doi:10.1371/journal.pone.0109373.
- Yang J-C, Ma X-Y, Xia H, et al. Clinical application of computer-aided design-rapid prototyping in C1-C2 operation techniques for complex atlantoaxial instability. J Spinal Disord Tech. 2014;27(4):E143-50. doi:10.1097/01.bsd.0000450173.95940.ed.
- Yddal T, Cochran S, Gilja OH, Postema M, Kotopoulis S. Open-source, high-throughput ultrasound treatment chamber. Biomed Tech (Berl). 2014. doi:10.1515/bmt-2014-0046.
- Zhang C, Anzalone NC, Faria RP, Pearce JM. Open-source 3D-printable optics equipment. PLoS ONE. 2013;8(3):e59840. doi:10.1371/journal.pone.0059840.
Bibliography - Internet
(A selection of recent internet press releases/news pieces on the topic)
- http://ir.rganovo.com/news/press-releases/press-releases-details/2014/Organovo-Announces-Commercial-Release-of-the-exVive3D-Human-Liver-Tissue/
- http://www.3ders.org/articles/20140421-comparing-50-dollar-3d-printed-hand-vs-42000-dollar-prosthetic-limb.html
- http://www.3ders.org/articles/20140610-3d-systems-unveils-3d-printed-bespoke-braces-for-better-treatment-of-chronic-scoliosis.html
- http://www.3ders.org/articles/20140723-metamason-revolutionizing-3d-printed-custom-cpap-masks-for-sleep-apnea-treatment.html https://www.qut.edu.au/about/news/news?news-id=72257