Association of Genetic Variants with Postsurgical Pain: A Systematic Review and Meta-analyses
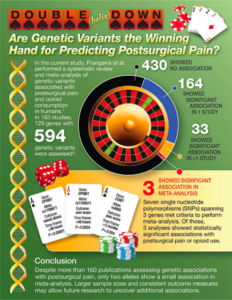
A new study in Anesthesiology examines the association between genetic variants and their possible association with postsurgical pain. Provoking study with results that may be a bit surprising.
Read the study here: https://pubs.asahq.org/anesthesiology/article/doi/10.1097/ALN.0000000000004677/139139/Association-of-Genetic-Variants-with-Postsurgical
Comparing Hemidiaphragmatic Paralysis In Various Approaches to Brachal Plexus Nerve Blockade

Hemidiaphragmatic paralysis is a known consequence of brachial plexus blockade, with pre-existing respiratory disease sometimes being a contraindication to considering such blocks. This meta-analysis assessed the impact of various approaches to brachial plexus blockade with the costoclavicular approach with positive findings that may impact clinical practice.
Read the study here: https://ekja.org/upload/pdf/kja-22718.pdf
The 2024 Rita Allen Foundation Scholars Award in Pain

The Rita Allen Foundation has provided a special award for early-career leaders in basic pain research whose work holds high potential for uncovering new pathways to improve the treatment of chronic pain. The Foundation has awarded annually two grants or more in the amount of $150,000 over three years to early-career investigators pursuing innovative research that focuses on basic science mechanisms of pain. Candidates should be in the early stages of their career with an appointment at the faculty level. More information about applying for this award, offered in partnership with the U.S. Association for the Study of Pain (USASP), including a link to the application portal as well as detailed application guidelines and instructions, can be found on the USASP website: https://www.usasp.org/rita-allen-foundation-award-in-pain. Applications are due December 14, 2023.
Question of the Month – December 2023
A 15-year-old, female, softball player presents for left knee ACL reconstruction with autograft, following a knee injury few weeks ago. The patient denies any numbness or weakness in her leg at this time, but active knee movement is limited by pain. Her past medical history and physical exam are otherwise unremarkable. Strength is perceived as 5/5 in all muscles tested. Sensation was normal in the affected lower extremity. For pain management, left femoral nerve block is done with 0.2% ropivacaine (10 ml) under ultrasound guidance, and femoral catheter left in place, after anesthesia induction, prior to surgical incision. iPACK block is done at the end. GETA is otherwise uneventful and surgical tourniquet time is noted to be 92 minutes. In the recovery room, she is pain-free. She is discharged home with nerve catheter in place infusing 0.15% ropivacaine @8 ml/hr with instructions for catheter care. She was followed by pain service while catheter is in place, and removal at home on postoperative day 3. Over this time there were no motor deficits reported. On routine post-surgical follow up 2 weeks after surgery in orthopedic clinic, she complains of persistent numbness in medial aspect of knee to foot. On exam, she also has weakness 3/5 with knee extension and has been unable to participate in physical therapy. The orthopedic surgeon refers the patient to the anesthesiologist who performed the block for further assessment. After a thorough exam and discussion, referral to neurology is placed. Electromyography/nerve conduction studies are conducted a week later which reveal neurapraxia.
Please select which of the following features will most help make the diagnosis of neurapraxia:
Correct!
Wrong!
Question of the Month - December 2023
- « Previous Page
- 1
- …
- 3
- 4
- 5
- 6
- 7
- …
- 38
- Next Page »